Appendicectomy : Types, Indications, Steps, Postoperative care and Complications
Appendicectomy may be performed by conventional open operation or by using laparoscopic techniques. The first surgeon to perform deliberate appendicectomy for acute appendicitis was Lawson Tam, in May 1880. The patient recovered. It is recorded in 1736 that Claudius Amyand successfully removed an acutely inflamed appendix from the hernial sac of a boy.
Appendicectomy should he performed under general anaesthetic with the patient supine on the operating table. When a laparoscopic technique is to be used, a nasogastric tube should be inserted and the bladder must be empty (ensure the patient has voided before leaving the ward). Prior to preparing the entire abdomen with an appropriate antiseptic solution, the right iliac fossa should be palpated for a mass. If a mass is felt, it may, on occasion, be preferable to adopt a conservative approach (vide infra). Draping of the abdomen is in accordance with the planned operative technique, taking account of any requirement to extend the incision or convert a laparoscopic technique to open operation.
Conventional appendicectomy
When the preoperative diagnosis is considered reasonably certain, the incision that is widely used for appendicectomy is the so-called grid-iron incision (a grid-iron was a frame of cross-beams to support a ship during repairs). The grid-iron incision (described first by McArthur) is made at right angles to a line joining the anterior superior iliac spine to the umbilicus, its centre being along the line at McBurney’s point.
In the subcutaneous tissues an arterial twig from the superficial circumflex iliac artery usually requires ligation.
The external oblique is incised in the line of its fibres along the length of the incision.
The fibres of the internal oblique and transversus abdominis are split, and with suitable retraction the peritoneum is opened. If better access is required, it is possible to convert the grid-iron to a Rutherford Morrison incision (vide infra) by cutting the internal oblique and transversus muscles in the line of the incision.
In recent years, a transverse skin crease (Lanz) incision has become more popular, as the exposure is better and extension, when needed, is easier. The incision, appropriate in length to the size and obesity of the patient, is made approximately 2 cm below the umbilicus centred on the midclavicular—midinguinal line .
The external oblique aponeurosis, internal oblique and transversus muscles are split in the direction of the fibres and the peritoneum is opened. When necessary the incision may be extended medially, with retraction or suitable division of the rectus abdominis muscle.
When the diagnosis is in doubt, particularly in the presence of intestinal obstruction, a lower midline abdominal incision is to be preferred over a right lower paramedian incision. The latter, although widely practised in the past, is difficult to extend, more difficult to close and provides less good access to the pelvis and peritoneal cavity.
Rutherford Morrison’s incision is useful if the appendix
is paracaecal or retrocaecal and fixed. It is essentially an oblique muscle-cutting incision with its lower end over McBurney’s point and extending obliquely upwards and laterally as necessary. All layers are divided in the line of the incision.
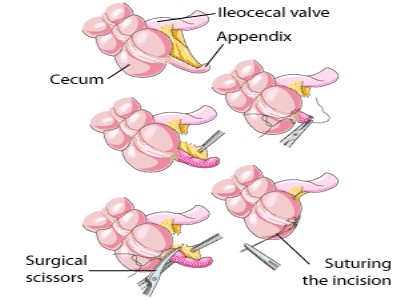
Removal of the appendix
It will be assumed that the abdomen has been opened by a skin crease incision. A retractor is placed under the medial side of the wound and the peritoneum, and the abdominal wall is elevated. Serous exudate is removed with a sucker. Pus, if present, is likewise removed having first retained a specimen for microbiological culture. The caecum is identified by the presence of teniae coli, and using a finger or a swab the caecum is withdrawn. A turgid appendix may be felt at the base of the caecum. Inflammatory adhesions must be gently broken with a finger which is then hooked around the appendix to deliver it into the wound. The appendix is conveniently controlled using a Babcock or Lane’s forceps applied in such a way as to encircle the appendix and yet not damage it. The base of the mesoappendix is clamped in a haemostat, divided and ligated . When the mesoappendix is broad the procedure must be repeated with a second, or rarely, a third haemostat. The appendix, now completely freed, is crushed near its junction with the caecum in a haemostat, which is removed and reapplied just distal to the crushed portion. An absorbable 2/0 ligature is tied around the crushed portion close to the caecum. The appendix is amputated between the haemostat and the ligature. An absorbable 2/0 or 3/0 purse-stringor ‘Z’ suture may then be inserted into the caecum about 1 cm from the base . The stitch should pass through the muscle coat, picking up the taeniae coli. The stump of the appendix is invaginated while the purse-string or ‘Z’ suture is tied, thus burying the appendix stump. Many surgeons believe that invagination of the appendiceal stump is unnecessary.
Methods to be adopted in special circumstances
When the caecal wall is oedematous, the purse-string suture is in danger of cutting out. If the oedema is of limited extent this can be overcome by inserting the purse-string suture into more healthy caecal wall at a greater distance from the base of the appendix. Occasions may arise when, because of the extensive oedema of the caecal wall, it is better not to attempt invagination.
When the base of the appendix is inflamed, it should not be crushed but ligated close to the caecal wall just tightly enough to occlude the lumen, after which the appendix is amputated and the stump invaginated. Should the base of the appendix be gangrenous, neither crushing nor ligation must be attempted. Two stitches are placed through the caecal wall close to the base of the gangrenous appendix, which is amputated flush with the caecal wall, after which these stitches are tied. Further closure is effected by means of a second layer of interrupted seromuscular sutures.
Retrograde appendicectomy
When the appendix is retrocaecal and adherent, it is an advantage to divide the base between haemostats. The appendiceal vessels are then ligated, the stump is ligated and invaginated, and gentle traction on the caecum will enable the surgeon to deliver the body of the appendix which is then removed from base to tip. Occasionally, this manoeuvre requires division of the lateral peritoneal attachments of the caecum.
Drainage of the peritoneal cavity
This is usually unnecessary provided adequate peritoneal toilet has been done. If, however, there is considerable purulent fluid in the retrocaecal space or the pelvis, a soft silastic drain may be inserted through a separate stab incision. The wound should be closed using absorbable sutures to oppose muscles and aponeurosis. In the presence of soiling or if a gangrenous appendix has been delivered through the wound, it is often wise to leave open or to delay primary closure by inserting a gauze wick between interrupted skin sutures (Brady) .
Laparoscopic appendicectomy
The most valuable aspect of laparoscopy in the management of suspected appendicitis is as a diagnostic tool, particularly in women of child-bearing age. In general, an open technique should be used to establish a pneumoperitoneum, and for insertion of the laparoscopic ports as it is safer than the closed techniques using a Verres needle. The placement of the operating port may vary according to operator preference and previous abdominal scars. The operator stands to the patient’s left and faces a video monitor placed at the patient’s right foot . A moderate Trendelenberg tilt of the operating table assists delivery of loops of small bowel from the pelvis. The appendix is found in the conventional manner
by identification of the caecal taeniae and is controlled using laparoscopic tissue-holding forceps. By elevating the appendix the mesoappendix is displayed . A dissecting forceps is used to create a window in the mesoappendix to allow the appendicular vessels to be coagulated or ligated using a clip applicator. The appendix, free of its mesentery, can be ligated at its base with an absorbable loop ligature , divided and removed through one of the operating ports. It is not usual to invert the stump of the appendix . A single absorbable suture is used to close the linea alba at the umbilicus and the small skin incisions may be closed with a subcuticular suture .
Patients who undergo laparoscopic appendicectomy are likely to be discharged from hospital and return to work slightly sooner than those who have undergone open appendicectomy, but it remains to be seen whether this justifies the slightly longer operating time and higher costs involved.
Problems encountered during appendicectomy
• A normal appendix is found — this demands careful exclusion of other possible diagnoses, particularly terminal ileitis, Meckel’s diverticulitis and tubal or ovarian causes in women. It is usual to remove the appendix to avoid future diagnostic difficulties, even though the appendix is macroscopically normal, particularly if a skin crease or grid-iron incision has been made. A case can be made for preserving the macroscopically normal appendix seen at diagnostic laparoscopy, although approximately a quarter of seemingly normal appendices show microscopic evidence of inflammation.
• The appendix cannot be found— the caecum should he mobilised and the taenia coli should be traced to their confluence on the caecum before the diagnosis of ‘absent appendix’ is made.
• An appendicular tumour is found — small tumours (under 2.0 cm in diameter) can he removed by appendicectomy; larger tumours should he treated by a right hemicolectomy.
• An appendix abscess is found and the appendix cannot he removed easily — this should be treated by local peritoneal toilet, drainage of any abscess and intravenous antibiotics. Very rarely a caecectomy or partial right hemicolectomy is required. (The first recorded operation for an appendix abscess was by Henry Hancock of Charing Cross Hospital, London, in 1848.)
Appendicitis complicating Crohn’s disease
Occasionally, a patient is operated on for acute appendicitis who is found to have concomitant Crohn’s disease of the ileo-caecal region. Providing the caecal wall is healthy at the base of the appendix, appendicectomy can he performed without increasing the risk of an enterocutaneous fistula. Rarely, the appendix is involved with the Crohn’s disease. In this situation a conservative approach may be warranted, and a trial of intravenous corticosteroids and systemic antibiotics used to resolve the acute inflammatory process.
Appendix abscess
Failure of resolution of an appendix mass or continued spiking pyrexia usually indicates that there is pus within the phlegmonous appendix mass. Ultrasound or abdominal CT scan may identify an area suitable for insertion of a percutaneous drain. Should this prove unsuccessful, laparotomy through a midline incision is indicated.
Pelvic abscess
Pelvic abscess formation is an occasional complication of appendicitis and can occur irrespective of the position of the appendix within the peritoneal cavity. The most common presentation is a spiking pyrexia several days following appendicitis; indeed the patient may have already been discharged from hospital. Pelvic pressure or discomfort associated with loose stool or tenesmus is common. Rectal examination reveals a buggy mass in the pelvis, anterior to the rectum, at the level of the peritoneal reflection. Pelvic ultrasound or CT scan will confirm. Treatment is transrectal drainage under general anaesthetic.
references: Bailey and Love Short Practice of Surgery
This is may help you

